Coronavirus in India: CDDEP-John Hopkins report estimates between 12.5 and 24 crore Indians to fall sick
Though the report puts India’s hospitalisation requirement at 25 lakh in a worst case scenario, that is about 1% of the total numbers of patients they have estimated, way less than the global figures


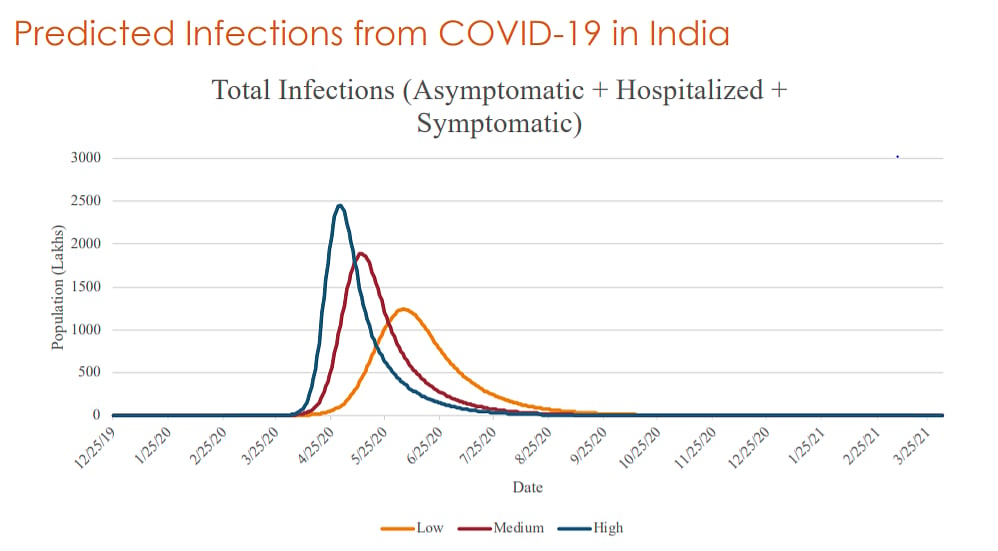
The Center for Disease Dynamics, Economics & Policy (CDDEP), a public health research organisation with headquarters in Washington, D.C. and New Delhi, has come out with a report on Coronavirus in India in collaboration with John Hopkins University, US. It has said that India was likely to see as many as between 12.5 crore to 24 crore of its people being infected with the deadly COVID-19 virus in the best and worst case scenarios respectively. In the best case scenario with decreased virulence, the peak will be around mid June, 2020 where as in the worst case scenario where government interventions like rate of testing and social distancing fails, the worst peak phase will arrive at around April 25, 2020. The study sees the effect of COVID-19 taper off August onwards.
But surprisingly, in its worst estimate it put India’s total hospitalisation requirement at just 25 lakh which is nearly one per cent of the total cases. Internationally COVID-19 has seen well over a 10 per cent hospitalisation rate. In that case, India’s health sector which provides for 1 hospital bed per 2000 people and less than 1,00,000 ICUs and ventilators nationwide could come under severe pressure.
The state level estimates put Uttar Pradesh and Maharashtra as the two most-affected states in India. The state level estimates were driven by date of seeding of the epidemic based on available testing data, presence of major metro cities where initial transmission is more rapid, flight connections to Covid19-affected countries and age and demographic variables.
The report said, “We use IndiaSIM, a well-validated agent-based model of the Indian population. This has been published widely over many years and has been used for government decision-making including by NTAGI for vaccine introduction. A brief summary of the model is attached. The model describes the actual Indian population in full detail of demography (age, gender), location, socio-economic characteristics and access to healthcare. Our unit of analysis is an actual simulated Indian and estimates are reliable down to the district level. The model is fitted to the most recently available NFHS and census data and uses state-of-art agent-based modeling methods.”
The report also made several observations. They are:
“1. Delays in testing are seriously reducing the ability of the population to protect itself. This is the most important way in which we can contain the epidemic. An increase in the official number of detected cases in the short term could encourage the population to take distancing more seriously and will reduce panic compared to a big spike later.
2. Border closures at this stage have little to no impact and add further economic disruption and panic. While international transmission was important in the first stage, domestic transmission is now far more relevant.
3. A national lockdown is not productive and could cause serious economic damage, increase hunger and reduce the population resilience for handling the infection peak. Some states may see transmission increase only after another 2 weeks and lockdowns should be optimized for when they could maximize the effect on the epidemic but minimize economic damage. State level lockdowns in the most affected states could change the trajectory of the epidemic and should commence immediately. Any delay allows for more secondary cases to emerge. Lockdowns should be guided by testing and serological survey data and should be planned on a rolling basis. We will expand these recommendations shortly.
4. Preparedness for case load should be the highest priority at this time. We will be issuing guidance based on the model for state level needs for bed capacity, oxygen flow masks and tanks and ventilators.
5. Temperature and humidity increases should help us in reducing case load. Although the evidence is limited, it is plausible.
6. We need to focus on both children under the age of five and the elderly. Early testing and healthcare in this population could help significantly reduce the mortality toll of the epidemic.
7. We should be prepared for multiple peaks in the model (we have only shown what happens in July) and we should be prepared for more cases and deaths later in the year.”
Follow us on: Facebook, Twitter, Google News, Instagram, WhatsApp
Join our official telegram channel (@nationalherald) and stay updated with the latest headlines