Suicides a public health emergency now
More children under the age of 18, more girls than boys, are dying by suicide than ever before; and so are daily wage earners and undertrials



The National Crime Records Bureau (NCRB), an agency under the Ministry of Home Affairs, last week published the national suicide data for 2021. The NCRB should be commended for publishing this data quickly, given all the pandemic-related restrictions that have affected functioning of many organizations.
Unfortunately, the suicide data for 2021 makes for very grim reading. Suicides in India increased by 7.2% in 2021 in absolute numbers and the suicide rate increased by 6.2%. This is extremely worrying as this increase comes after 10% increase in suicides and an 8.7% increase in the suicide rate in 2020.
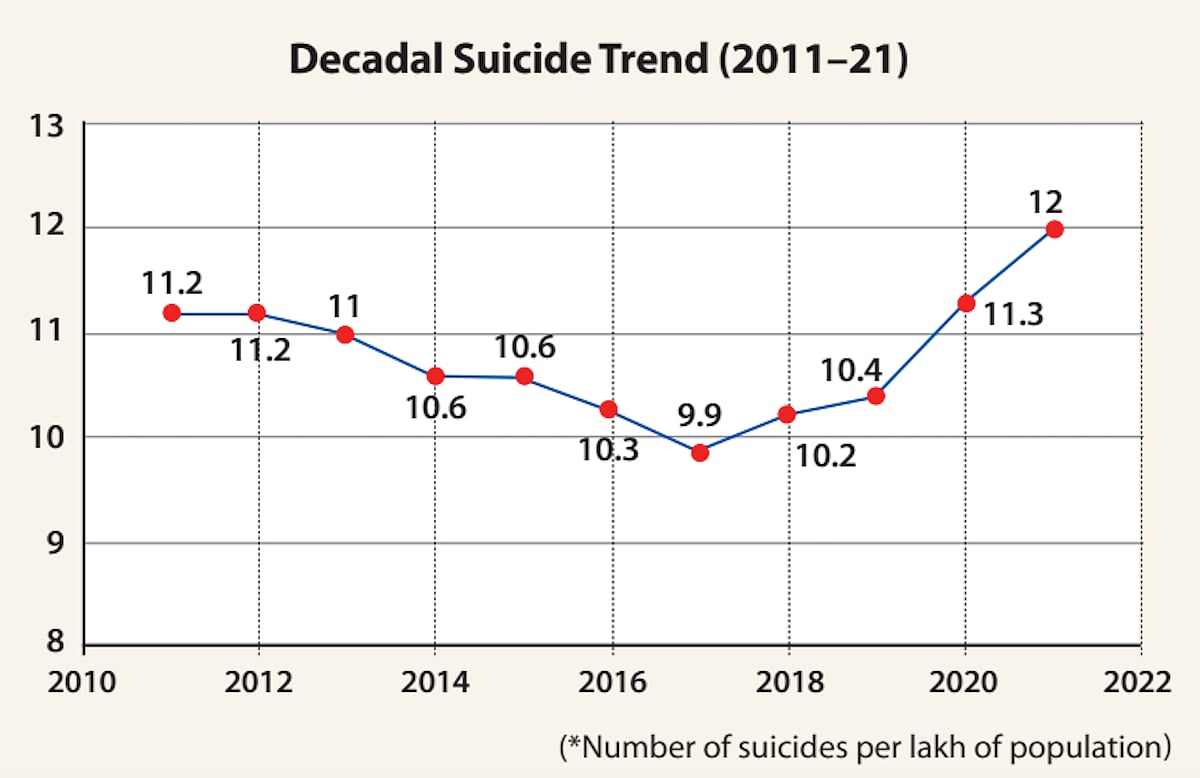
To put this in context, suicides steadily reduced from 135,585 suicides in 2011 to 129,887 in 2017 and the suicide rate decreased from 11.2 in 2011 to 9.9 in 2017. However, since then, suicides have steadily increased by 26% in four years, with nearly 18% of this increase happening in the past two years (2020 and 2021). India’s suicide rate for 2021 is at 12 ((calculated per lakh of population), which is higher than the rate of 11.2 in 2011.
We also know from research studies in the past 15 years, that NCRB data under-estimates the real number of suicides by 30% to 100%, so real number of suicides in India is likely to be significantly higher than the NCRB number.
There are three population sub-groups where the data is particularly worrying. The first group is children under 18 years. Suicides in children increased by 18.5% in 2020, the pandemic year (when total suicides increased by 8%). In 2021, fortunately suicides in children have decreased by approximately 6% but continue to remain above 10,000 suicides per year. This is the only age group where girls outnumber the boys in suicide deaths for past many years (in other age groups, men outnumber women by a wide margin).
We need to understand why such a high number of children are dying by suicides each year and what can be done to reduce suicides in children. It would be tempting to blame this entirely on exam failures, but the data shows that exam failures barely account for 10% of children suicides and the vast majority of children’s suicides are attributed to ‘family problems’.
Another sub-group that needs particular attention is daily wage earners. While total suicides increased from 131666 to 164003 (a 25% increase) from 2014 to 2021, suicides by daily wage labourers increased from 15735 in 2014 to 42004 in 2021, a 167% increase. Suicides among daily wage earners are increasing nearly 6 times faster than in the rest of the population.
The third group which has attracted little attention is suicides amongst prisoners. Since 2017, NCRB has released data on prisoners dying by suicide. As the chart below shows, suicide rates amongst prisoners are two to three times the national suicide rate.
Faced with these grim numbers, there will be an urge to implement knee-jerk solutions and our policy makers should refrain from such actions. Suicides are not going to drop dramatically with one or the other intervention done for a few weeks or months.
If policy makers are genuinely committed to reducing suicide rates in India, they need to develop and implement an integrated Suicide Prevention Policy and Strategy. While a national suicide prevention strategy is necessary, it is important to remember there are significant regional variations in suicides and the population sub-groups at risk throughout the country, states need to develop and implement their own state suicide prevention policies and strategies to address the suicides profiles in their own states.
Suicides are caused by a multitude of factors and thus any suicide prevention strategy needs to be inter-sectoral involving many sectors such as education, agriculture, employment, social justice (domestic violence prevention) along with the health and mental health sector.
A suicide prevention strategy also needs targets for 3, 5, 7 years for example. Suicide rates are likely to drop only with a time lag with the implementation of effective strategies and hence a longer time horizon for evaluating the success or failure of strategies is needed.
Monitoring targets also highlights the need for good quality suicide data. It is a historical anomaly that suicide data is collected by NCRB, which is a police agency. We should move suicide data collection responsibilities to a public health agency with an emphasis on collecting data to understand the psycho social causes of suicides.
We also need to rectify another glaring omission in our data collection. While we collect data on suicides (however poorly it is done), we do not systematically collect national data on attempted suicides. In most countries, attempted suicides range from 4 to 20 times the number of deaths by suicides. Using this metric, India is likely to have anywhere between 0.6 million to 3.2 million attempted suicides each year based on the NCRB suicide data.
Attempted suicides are the single best predictor for a future death by suicide. Thus, this is a high-risk group which needs immediate intervention and provision of services to this high risk group carries the potential for reduction in suicides in the coming years.
It is important that policy makers adopt evidence-based interventions for suicide prevention. For example, the World Health Organization recommends countries adopt 4 evidence-based interventions – reduce access to means of suicide, responsible media reporting of suicides, fostering life-skills development in adolescents and early identification, management and follow up of individuals with suicidal behaviours.
India would do well to invest resources and efforts on these four strategies to start with. In addition, specific strategies may be required for certain sub-groups where socio-economic factors may play a significant role, for example farmers and daily wage earners.
Suicides are number one cause of death in young women and number two cause of death in young men in India. Suicides have become a public health emergency and require immediate attention from our policy makers at the central and state level. A National Suicide Prevention Agency, modelled on the lines of NACO for HIV/AIDS prevention and control is required to co-ordinate suicide prevention actions between different sectors. Such national agency also needs to be well resourced and led by public health experts with experience in suicide prevention to ensure we can implement suicide prevention strategies effectively.
(Dr. Soumitra Pathare is a clinical psychiatrist and Director, Centre for Mental Health, Law and Policy at the Indian Law Society, Pune)
Join our official telegram channel (@nationalherald) and stay updated with the latest headlines
Published: 09 Sep 2022, 5:00 PM